Save to my favorites
What is it?
Abdominal flap reconstruction is a surgery that uses part of your abdomen (outer stomach area) to make a new breast.
There are a few different ways to perform this surgery, but all of them use some combination of skin and fat from the abdomen to reconstruct your breast.
The two different kinds of surgeries we will talk about are:
- Pedicle TRAM Flap
- Takes skin, fat, and muscle from the lower abdomen
- DIEP Flap (pronounced “Deep”)
- Takes skin and fat from the lower abdomen, and does not take muscle
- You may have a faster recovery with this surgery, compared to other abdominal flap surgeries
Learn more about the different abdominal flap surgeries:
Pedicle TRAM
- Skin, fat, and part of the “six-pack” muscles are tunneled up to the mastectomy site and shaped into the new breast
- A portion of the muscle is still attached to the stomach area
- The blood vessels are still connected
DIEP Flap
- DIEP flaps are made up of abdominal skin, fat, and blood vessels from your lower abdomen
- None of the six-pack muscle is removed
- The surgeon reconnects blood vessels from the flap with vessels along the breastbone or in the armpit
How is it done?
The surgeon uses skin, fat, and (sometimes) muscle from your stomach area to make a new breast.
Learn more about the steps
Start
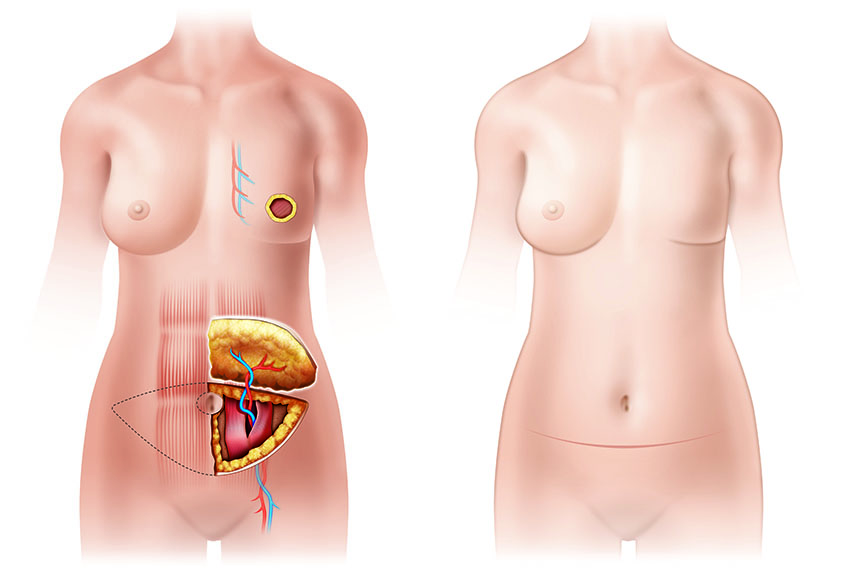
Natural Tissue Transfer
- The surgeon moves issue from your abdomen to the breast being reconstructed
- This can happen at the same time as your mastectomy or later
- Your skin provides the covering, and the fat is the filler for your new breast
- The cut on your lower abdomen usually runs from hip to hip, but the scar is low enough to be hidden by many types of swim suits
3 Months
Nipple Reconstruction or other optional procedures
By the numbers
- Number of surgeries:1 or more
Many patients also have a later surgery to re-shape the breast.
- Nights in the hospital:2 to 5
This type of reconstruction is a major surgery, so the amount of time you will spend in the hospital after the operation will be longer compared to other kinds of reconstruction.The number of nights ranges from 2 to 5, depending on the specific procedure (how the abdominal tissue is used to reconstruct your breast).
- Length of recovery:6 to 10 weeks
You should not drive for 4 weeks after your surgery. Physical work and exercise are restricted for 6 weeks. Most people need more time (often another month) to resume normal activities, especially if their job is physically demanding.Even after the initial recovery time has passed, you still may not feel like yourself. You may still feel tired and sore for a few months after your surgeries.
What are the pros?
- No implant risks
You will avoid the potential risks of implants, such as scar tissue formation and leakage.
- Better matching with the opposite natural breast
The tissue from the stomach area can be shaped and molded to better match your opposite natural breast, and you will less likely need surgery on the opposite breast.Breasts reconstructed from abdominal tissue are soft (similar to natural breast tissue) and have a more “mature” shape, which will “sag” more naturally over time to match the opposite breast.
- Works well for patients who had radiation
Abdominal flap reconstruction moves new tissue and blood circulation to the radiated area. This helps improve healing and may lower your chances of getting an infection.
- Changes to match body weight
Because the reconstructed breast is mostly made of fat from the stomach area, it’s size will increase or decrease with weight gains or losses, much like a natural breast would. This lowers the chances of having unequal (or lopsided) breasts later in life.
What are the cons?
- Longer surgery, hospitalization, and recovery
Flap reconstruction is a major surgery, which means the operations are longer and require a hospital stay for a few days after the procedure. These surgeries also usually require several months for full recovery.
- May not be an option for women that are very over- or underweight
For women who are very overweight, there is a higher chance that the stomach tissue that is moved to your breast will “fail”.A failure occurs when part or all of the tissue that was moved dies, usually due to poor circulating blood flow to the newly reconstructed breast. This will be explained in more detail in the section “What are the risks”.For very thin women, there may not be enough fat in the stomach area to perform this type of reconstruction.
- More invasive I Leaves scars in the stomach area of your body
A cut will be made at the donor site (where the stomach tissue is taken from). This will cause an extra scar on your body in addition to the scar from your mastectomy.Even though the scar at the donor site is in the lower part of your stomach area, it may still limit some choices in clothing, like swimwear.
What are the risks?
- Circulation (blood flow) problems I Transferred tissue failure
- Abdominal flap reconstruction can have circulation problems in the first few days after surgery. These problems with blood flow can sometimes lead to transferred tissue failure, or flap loss.
There are different rates of transferred tissue failure (flap loss) between different surgeries:
Pedicle TRAM Flap:
Total flap losses happen in 1% of women (1 out of 100)Partial flap losses (portions of skin or fat) happen in about 7% of women (7 out of 100)
DIEP Flap:
Total flap losses happen in 2% of women (2 out of 100)Partial flap losses (portions of skin or fat) happen in about 10 to 15% of women (10 - 15 out of 100)
- Infection
- Infection rates after surgery are 3 to 4% of people (3 - 4 out of 100).
- Bleeding or fluid collection
- Chances of abnormal bleeding after surgery are about 2% of women (2 out of 100)
- Hernias or bulges in stomach area
- Abdominal hernias or bulges happen in about 7% (7 out of 100) Pedicle TRAM flap surgeries,and 2% (2 out of 100) DIEP Flap procedures.
- May weaken stomach muscles (Pedicle TRAM only)
- Patients having reconstruction with the pedicle TRAM procedure will require parts of the “six pack” muscles to be moved.
This may cause the stomach muscles to be weaker (sit up power), and may also make it hard to get back to normal activities.
The impact on the stomach muscles is less for patients having reconstruction on only one side with this procedure.
Possible major complications
- Re-operation | Re-hospitalization | Reconstruction failure
- In general, there is a 27 to 30% chance of having a major complication after abdominal flap reconstruction. That means 27 - 30 women out of 100 will need one of the following:
- Re-operation (needing to have another, unexpected surgery)
- Re-hospitalization (needing to be admitted back into the hospital after surgery)
- Reconstruction failure (the reconstruction doesn't work)
You may be at higher risk for complications, based on what you told us about yourself:
- Your BMI (Body Mass Index) is 35 or higher
- You currently smoke
- You are over 60 years old
Learn more about your risk of complications:
Your personalized risk*
Reconstruction using your own tissue
- If you have a flap-based reconstruction, your risk of a major complication would be 29%.
This means 29 out of 100 women like you have a major complication after flap-based reconstruction.
* This information is only an estimate. Everyone is different, and your risk might be different from what's shown here. Talk with your doctor for more information.
How do other women feel about it?
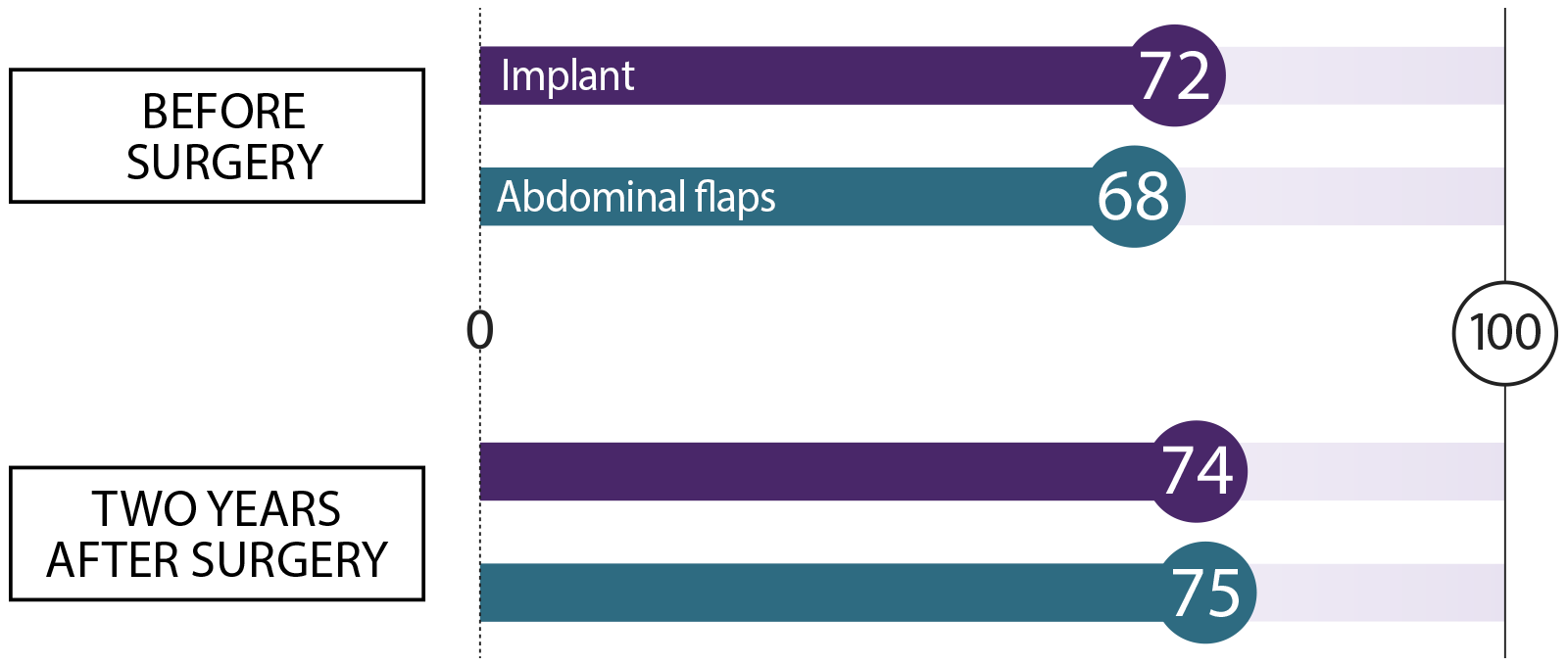
We asked women who had breast reconstruction how they felt before surgery and two years after their procedure. We asked about these topics. Here’s what they said:
Satisfaction with breasts How happy are you with the look and feel of your breasts?
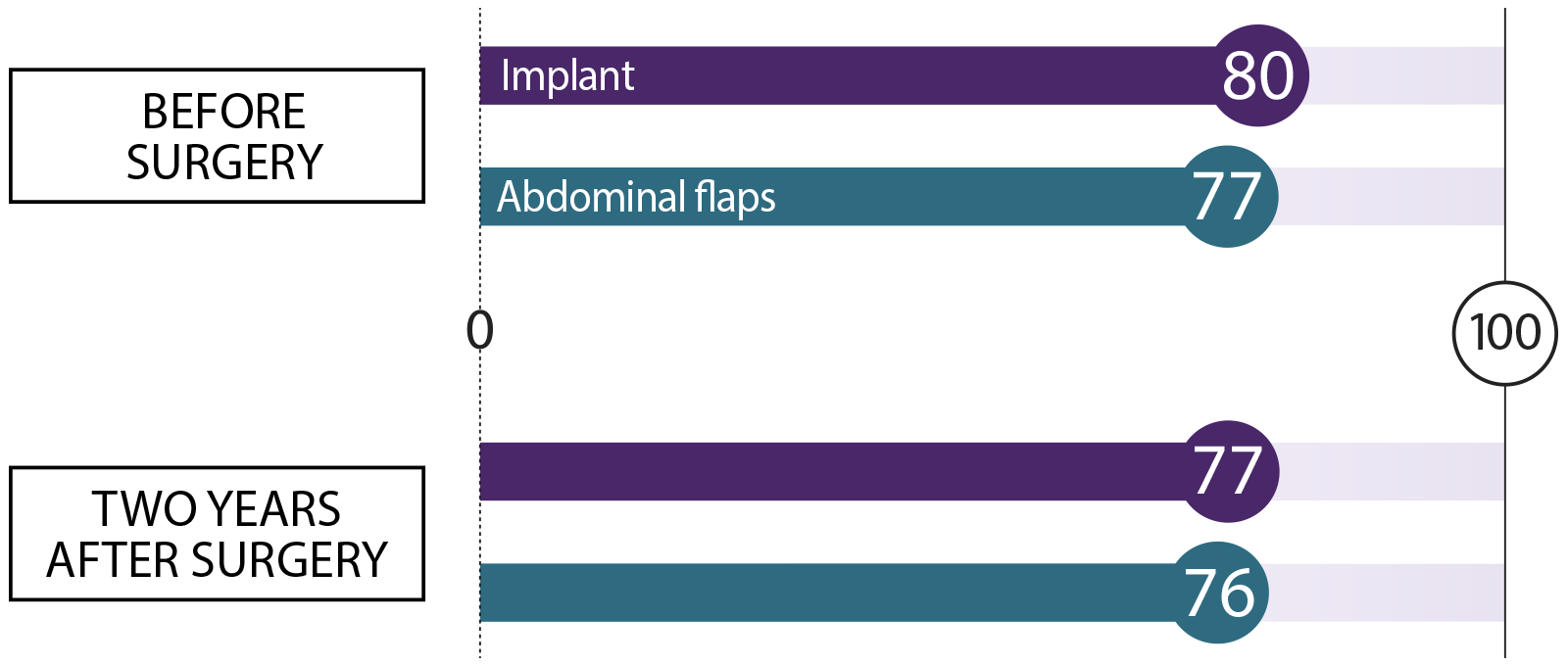
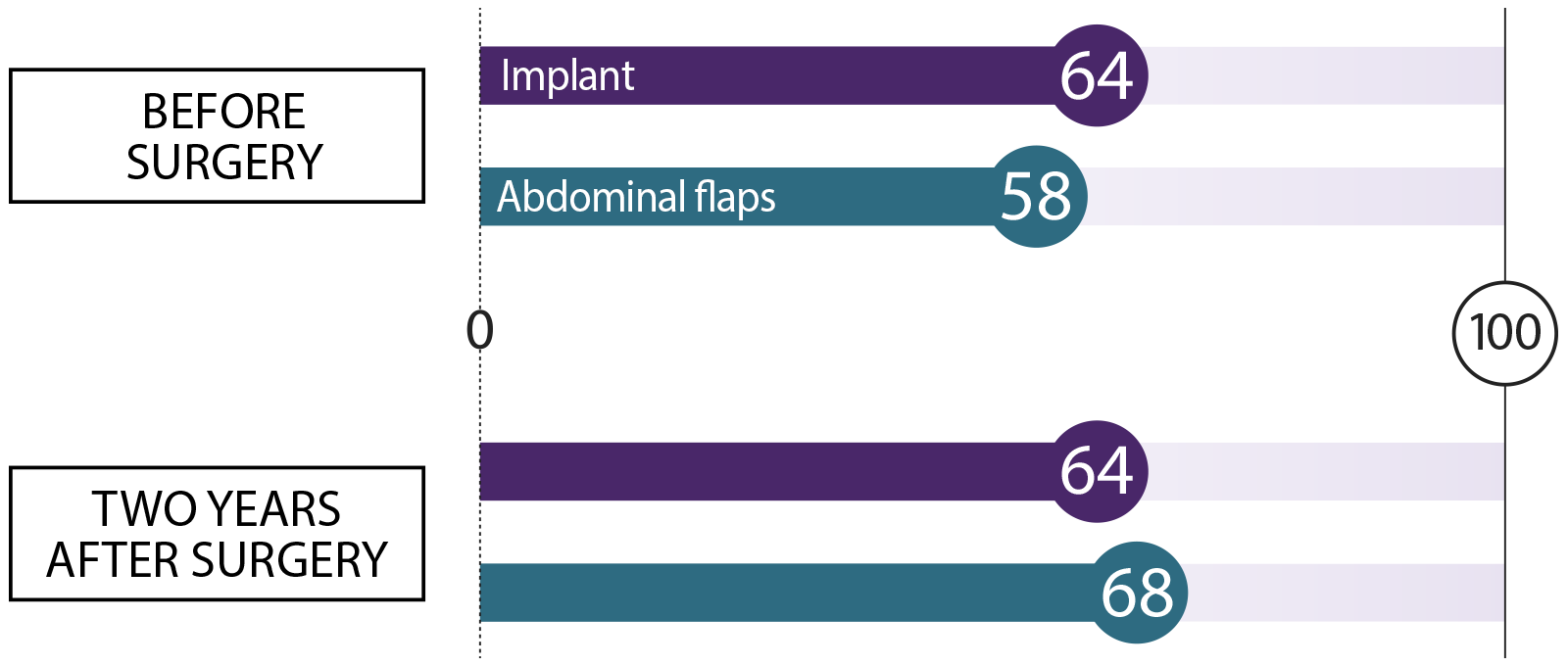 Sexual well-being
Sexual well-being How do you feel about your body as it relates to your sexuality?
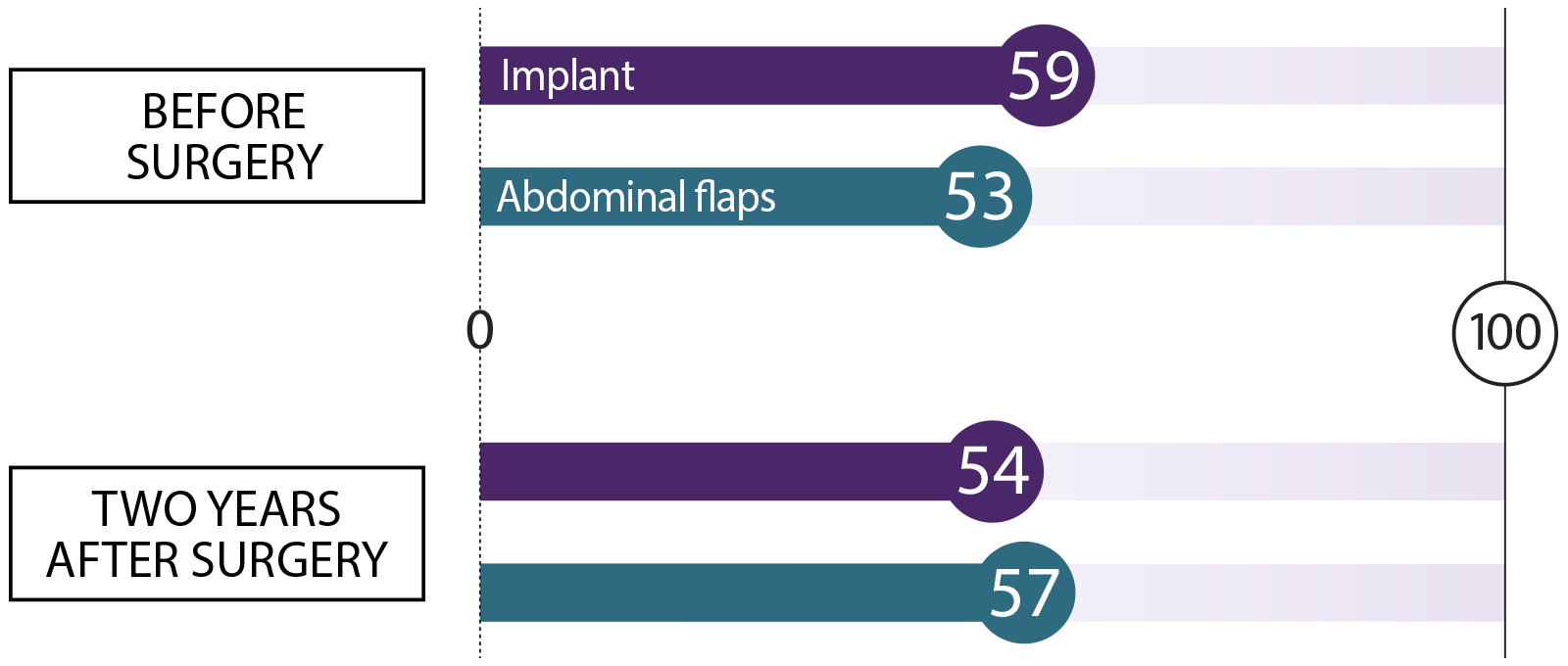 Psychosocial well-being
Psychosocial well-being How do you feel about your body image, and how confident are you in social settings?
 Physical well-being: Chest
Physical well-being: Chest How does your chest feel, physically?
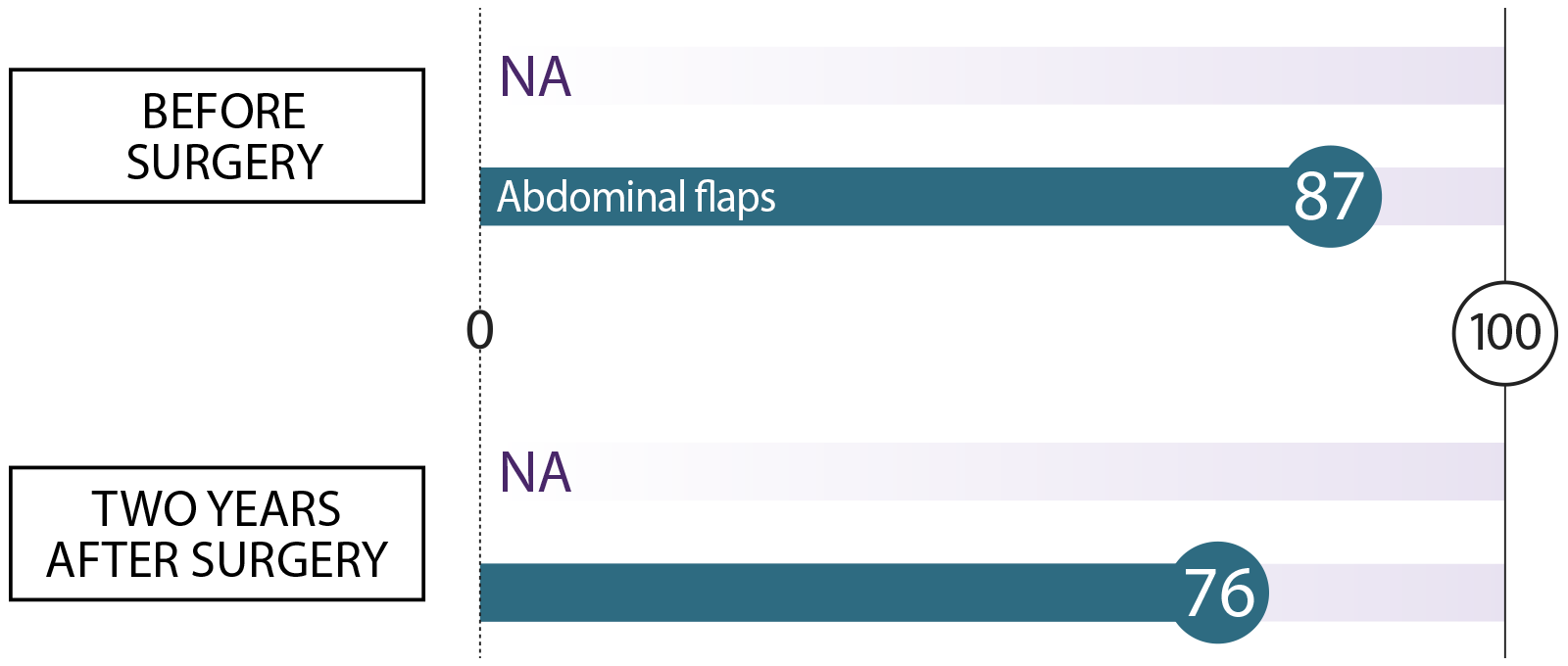
 Physical well-being: Abdomen
Physical well-being: Abdomen How does your abdomen (stomach area) feel, physically?